

- Scapula fractures are uncommon and they only result from high energy trauma because scapula is in protected position
- Common causes include:
- Direct blunt trauma
- Crush injuries
- Fall on the shoulder
- Seizures
Scapula anatomy
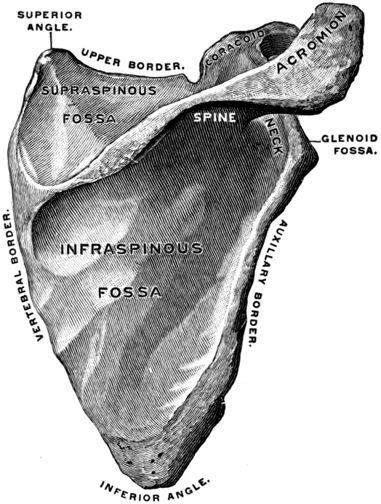
- Scapula (aka shoulder blade) is a triangular flat bone located on the posterolateral aspect of the thorax
- The posterior surface of scapula is divided by a thick ridge of a bone which is called the spine of scapula
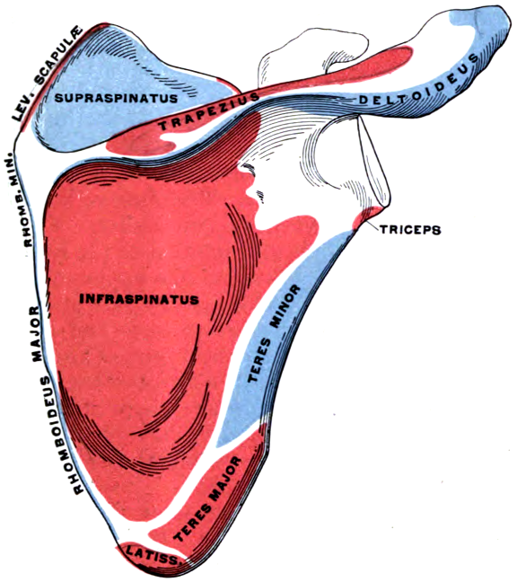
- It is divided into a smaller supraspinous fossa (origin of supraspinatus muscle) and a larger infraspinous fossa (origin of infraspinatus and teers minor muscles)
- The spine of scapula continues laterally to form the acromion, acromion articulates with the acromial end of the clavicle and it is also a point of attachment to trapezius muscle
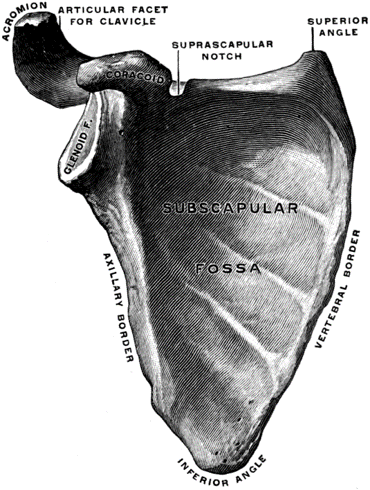
- The anterior surface of scapula forms the subscapular fossa (origin of subscapular muscle
- Superolateral of the scapula, there is the glenoid cavity, which articulate with the head of the humerus at the glenohumeral joint
- Superior to the glenoid, there is the coracoid process which projects anterolaterally, it provide attachment to CC ligaments, and it is the origin of the short head of biceps and brachialis muscles

Clinical features
- Patient arm is held immobile and there is severe bruising over the scapula and the chest wall due to the high energy injury sustained by that area
- Patient complain of severe diffused shoulder pain, shortness of breath and chest wall pain
- Evaluate and resuscitate patient based on ATLS trauma protocol
- There is usually associated severe injuries to the chest, brachial plexus, spine, abdomen and head, look for them
- Careful neurological and vascular examinations are essential
Imaging
- In addition to trauma labs and radiographs, send the patient for Scapula AP and Y views and shoulder axially view are the most helpful radiographs in detecting scapula fractures
- But these fractures might be difficult to be seen on X ray due to surrounding soft tissues
- CT scan are useful in detecting and classifying scapula fractures and detecting associated injuries
Classification
- Fractures of the scapula are classified anatomically into:
- Fractures involving scapular body
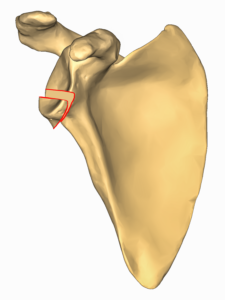
- Isolated glenoid neck fractures (extraarticular)
- Intra articular glenoid fractures
- Fractures involving acromion
- Fractures involving coracoid
- Last 3 types are subclassified into different grades
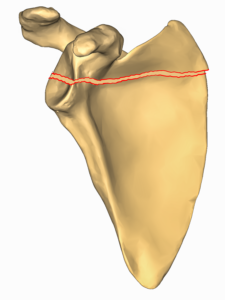
Scapular body fractures classification
- Scapular body fractures are described based on anatomical location
- Most of these fractures are minimally displaced and treated non operatively with sling immobilization
- Patient is advised to exercise the shoulder, elbow and fingers from the beginning to prevent stiffness
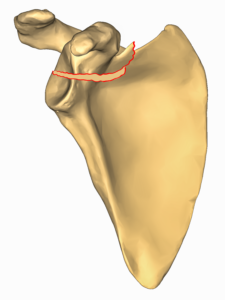
Isolated glenoid neck fractures classification
- This is one of the more common fractures involving scapula
- They are extra articular (don’t involve the glenohumeral joint)
- CT scan is required to make sure that the fracture is not intraarticular
Intraarticular Glenoid fractures classification
- Fractures involving the glenoid fossa and rim are subclassified according Ideberg modified by Goss classification
- This is the most commonly used classification to describe Glenoid fractures
Ideberg modified by Goss classification
Type I
- Fracture involving the glenoid rim
- Mostly minimally displaced and treated non operatively
- If the fracture involve more than a 25% of the glenoid surface and is displaced by 5 mm then this is indication of surgical fixation of Type I fractures

Type II
- Fracture through glenoid fossa
- Inferior fragment significantly displaced, The attached long head of the triceps may drag the fractured glenoid downwards and laterally
- Associated with humeral head subluxation => unstable shoulder joint
- Treatment is with open reduction and internal fixation since shoulder joint is unstable
Type III
- Oblique fracture through the glenoid exiting superiorly
- Significant displacement
- Maybe associated with AC joint dislocation
- Treatment: If the humeral head is centered on the major portion of the glenoid and shoulder is stable then a non operative approach is taken but if not then treated operatively
Type IV
- Horizontal fracture exiting through the vertebral border of the scapula
- Significant displacement
- Treatment: If the humeral head is centered on the major portion of the glenoid and shoulder is stable then a non operative approach is taken but if not then treated operatively
Type V
- Combination of type IV and another fracture separating the inferior part of the glenoid
- Significant displacement
- Treatment: If the humeral head is centered on the major portion of the glenoid and shoulder is stable then a non operative approach is taken but if not then treated operatively

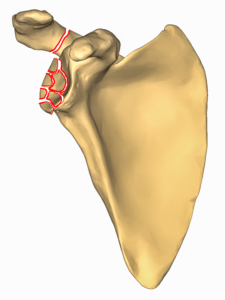
Type VI
- Severe comminution of the glenoid surface
- Significant displacement
- Treated operatively
Fractures involving acromion classification
- Classified according to Kuhn acromial fracture classification, this classification include three types:
- Type I minimally displaced => treated non operatively
- Type II displaced but does not compromise the subacromial space => treated non operatively
- Type III displaced and compromises the subacromial space => treated operatively
Fractures involving coracoid classification
- Those classified according to Ogawa coracoid process fracture classification, it is on two types:
- Type I fracture occurs proximal to the coracoclavicular ligament => associated with AC joint separation => mostly treated operatively
- Type II fracture occurs distal to the coracoclavicular ligament => doesn’t hurt AC joint => treated non operatively
Combined fractures
- If there was a fracture involving the scapula + there is associated fracture of the clavicle or disruption of AC ligament => glenoid gets displaced => it is called “ the floating shoulder”
Scapulothoracic dissociation
- Disruption of the scapulothoracic articulation where the scapula is displaced by > 1 cm from the spinous processes in comparison with the contralateral side
- It is caused by high energy trauma
- Associated with severe neurovascular injuries and fractures
Complications
- Post traumatic glenohumeral arthritis: high risk for this if it was intra articular glenoid fractures
- Malunion
- Recurrent glenohumeral instability
- Neurovascular injury
Course Menu
This article is apart from the Shoulder and Arm Trauma Free Course, which contain 10 lectures listed down below: