
- Radius and Ulna shaft fractures occur commonly
- The radius and ulna are linked together, so they get fractured together in most cases. But a fracture to a single bone can occur in some cases
- Most of the single bone fractures (either radius or ulna) are associated with a another injury at another level but some of them occur in isolation
- Examples of a single bone forearm fractures associated with a second injury:
- Monteggia fracture dislocation: ulnar shaft fracture with radial head dislocation
- Galeazzi fracture dislocation: radial shaft fracture with distal radioulnar joint injury
- Essex-Lopresti injury: radial head fracture with distal radioulnar joint injury
- Here we will explain both forearm bones fractures and the single isolated forearm bone fractures
Mechanism of injury
- A fall on the hand produces a spiral or transverse fracture of both bones usually
- A direct blow to the forearm causes a transverse fracture of just one bone (mostly the ulna)
- In high energy injuries, the fracture might be comminuted or segmental
- Additional displacement is achieved by muscle pull produced by the muscles attached to the radius and ulna, e.g. biceps, triceps, brachialis, supinator, pronator teres, and pronator quadratus
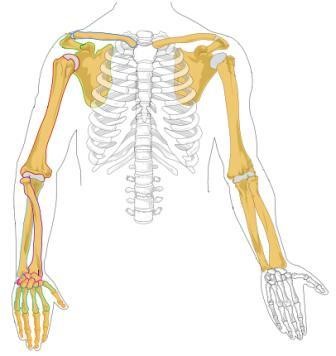
Anatomy
- The forearm consist of two bones, radius and ulna which articulate with each through two joints, one proximally through the proximal radioulnar joint and one distally through the distal radioulnar joint
- The whole forearm is considered a joint capable of rotation (pronation and supination)
- Fractures anywhere on the radius and ulna are considered intra articular fractures
- The radius and ulna also articulate through hinge joints with the humerus proximally and wrist distally
- These joints allow for flexion/extension type of movement, in addition the wrist joint allows for radial and ulnar deviation movements
- Loss of normal shape of radius or ulna during fractures will result in restriction of the normal pronation/ supination movements
- So these bones has to reconstructed perfectly, except in Pediatrics population because pediatrics bones tend to remodel well but still there is specific acceptable displacement criteria that has to be followed
- The muscles of the forearm are contained within compartments separated by fascial envelopes in narrow space (forearm) => there is a risk of compartment syndrome when pressure increases in these compartments especially in high energy injuries
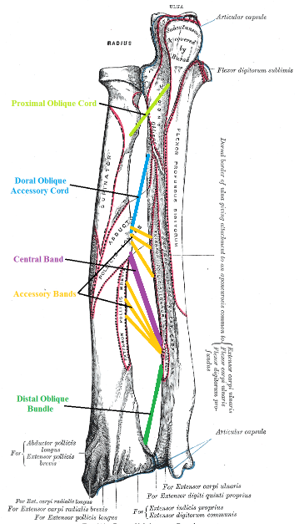
- Forearm ligaments include:
- The annular ligament in the proximal radioulnar joint
- The interosseous membrane in the mid forearm
- The triangular fibrocartilage complex in distal radioulnar joint
Neurovascular anatomy
- Anterior and posterior interosseous nerves
- Ulnar nerve
- Radial nerve
- Brachial artery divides into ulnar and radial arteries
- All of those are liable to injury during radial/ ulnar shaft fractures
Clinical features
- Symptoms
- Patient present with pain and deformity of the forearm
- Ask if there is pain in the wrist or elbow
- Physical examination
- Look
- Look for Swelling
- Deformity might be seen if there is severe displacement
- Inspect the lacerations for any evidence of open fracture
- Feel
- Feel for tenderness in the forearm , elbow and wrist
- Neurovascular examination is done to look for nerve/vessel injury
- Move
- Patient refuse movement due to pain
- Examination is repeated multiple times to exclude compartment syndrome
- Look
Imaging
- Plain radiographs (AP and lateral) are enough for diagnosis
- The radiograph should include the elbow and wrist to detect any injuries to the proximal or distal radioulnar joints

Treatment
- Non operative
- Operative
Non operative treatment
- It is done by closed reduction and immobilization
- Commonly done in pediatrics, and gives excellent results because periosteum is strong and guides reduction process
- Non operative treatment is rarely done in adult patients because it is difficult and result in unstable reduction, so operative treatment is superior in adults
- After closed reduction, The fracture is held in above elbow backslab (to prevent rotation) with elbow at 90 degrees and supported with sling
- In cases where the radius is fractured proximal to the pronator teres muscle insertion, the forearm is immobilized while supinated, while in cases where the radius is fractured distal to the pronator teres, the forearm is immobilized while being in the neutral position
- Neurovascular examination and plain radiographs are repeated shortly after reduction; Plain radiographs are repeated again after a week to make sure no further displacement occurred, and the forearm is immobilized for 6-8 weeks
- Exercises are started as soon as pain allows, including hand and shoulder exercises
Operative treatment
- Indications:
- Failure of closed reduction
- Unstable reduction
- Open fractures
- Operative treatment options include:
- percutaneous pinning
- ORIF with intramedullary nailing
- ORIF with plates and screws (most common)
- ORIF with K wire fixation
- ORIF is preferred in adults because reduction is difficult and redisplacement is common except if the fragments are in close contact to each other
- Deep fascia is left open to prevent compartment syndrome and only the skin is sutured
- After the operation, the arm is kept elevated until the swelling subsides and exercises are started as soon as possible
Complications
radius and ulna shaft fractures complications include early and late complications
Early complications
- Nerve injury: Nerve injuries in elbow dislocations are mostly iatrogenic occur during the surgery
- Vascular injury: radial or ulnar arteries can be injuried but it is of no problem since the collateral circulation will satisfy requirements
- Damage to the forearm muscles leading to bleeding and swelling, this may lead to higher pressures inside the muscle compartments, impaired circulation and compartment syndrome
Late complications
- Malunion: occur with closed reduction, there might be angulation, rotation or shortening
- Delayed union and non union: those are rare
- Complications of plate removal: those are common and they include nerve and vessel damage, infection and refracturing
- Synostosis (cross union): the forearm would be fixed and uncapable of rotation anymore
- Stiffness (intraarticular fractures)
Course Menu
This article is apart from The Elbow and Forearm Trauma Free Course; This course contains a number of lectures listed below: