
- Elbow dislocation is the second most common large joint dislocation in adults (up to 25%) and the most common large joint dislocation in children
- It mostly affect younger patients aged 10-20 years due to sports injuries and high energy injuries (e.g. road traffic accidents)
- That is because, the elbow is a highly stable joint, it requires a considerable amount of force to be dislocated
Anatomy
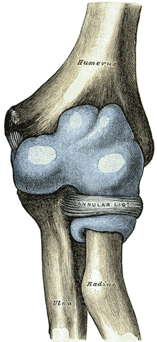
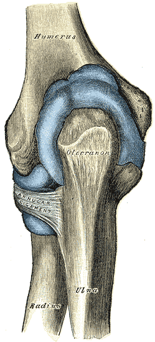
- Elbow is a hinge type of synovial joint
- It is formed by the articulation of the capitulum and trochlea of the distal humerus with the radial head and trochlear notch of the radius and ulna respectively.
- The articular surfaces of these bones are almost in full contact with each other leading to higher stability of the elbow joint
- The joint capsule of the elbow surrounds the elbow joint and provide more stability
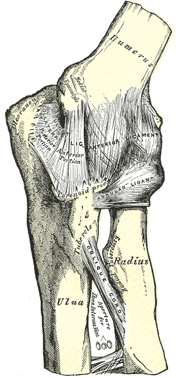
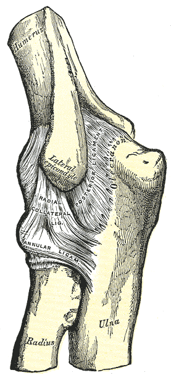
- Elbow joint is furtherly stabilized by ligaments, those include:
- radial collateral ligament: connect lateral epicondyle of the humerus with the annular ligament
- Annular ligament of the radius: encircles the radial head into the ulnar notch
- Ulnar collateral ligament: connects medial epicondyle of the humerus to the coronoid process and olecranon of the ulna and it contain two bands anterior and posterior
- Muscles around the elbow joint also help in stabilization (common flexors, common extensors, brachialis, triceps …)
- All of these factors make the elbow a highly stable joint but sometimes dislocation occur
Pathological anatomy
- When elbow dislocation occurs, this may lead to:
- Bony injury (radial head fracture, coronoid process fracture)
- Capsular injury
- Ligament injury (especially medial collateral ligament)
- Muscle injury
- In simple dislocations, there will be no bone injury but the capsule and ligaments will be injured, however the elbow will be reduced and it will still be stable after reduction
- In complex elbow dislocations, there will be bone injury in association with the capsular and ligamentous injuries; radial head being the most common associated fracture and coronoid process of the ulna being second most common, in these injuries were there is elbow dislocation and only one fracture (either radial head or coronoid process) then elbow will also be stable after reduction in most cases
- If all of these three come together (elbow dislocation + radial head fracture + coronoid process fracture) then this is called terrible triad injury and in this case elbow will be unstable after reduction with bad prognosis (recurrent dislocations and osteoarthiritis)
Classification
- Elbow dislocations are classified according to the direction of displacement of the forearm relative to the arm into posterior (90%), anterior, medial, lateral and convergent
- Elbow dislocations also classified into simple and complex, simple is without associated fracture and complex is with associated fractures (e.g. coronoid process fracture or radial head fracture)
Coronoid process fracture classification
- Ulnar coronoid process is classified according to Regan and Morrey classification
- Regan and Morrey classifies coronoid process fractures according to the size of the fractured fragment into:
- Type I: fracture of the tip of the coronoid process (small fragment)
- Type II: fracture of < 50% coronoid process fragment
- Type III: fracture of > 50% coronoid process fragment
Clinical features
- Symptoms
- Patient present with elbow pain and deformity, patient elbow is usually held in slight flexion and supported by the other hand
- Physical examination
- Look
- Elbow swelling
- There might be ecchymosis around the elbow
- Deformity is obvious
- Feel
- there is tenderness on pressure around the elbow, and bony landmarks (olecranon and epicondyles) maybe abnormally placed
- Check radial pulse and compare with other hand to make sure no vascular injury is sustained
- Neurological examination will reveal Ulnar nerve injury in most cases
- Move
- Patient refuse to move their elbow
- Look
Imaging
- Plain radiographs are enough for diagnosis, CT scan maybe required for surgical planning and assessment
- AP and lateral elbow x rays shows the dislocation well, radiocapitellar line is drawn to make it easier to spot the dislocation
- The challenge with plain radiographs is to identify the associated injuries
- The dislocation direction is described, also the associated fractures and injuries should also be described in the report

- In the x ray, the dislocation is divergent, in which there is ulnohumeral, radiohumeral and proximal radioulnar joints all dislocated
Associated injuries
- Radial head fracture
- Coronoid process fracture
- Terrible triad injury
- Medial epicondyle fracture (mostly in children)
Treatment
- Simple elbow dislocations are treated non operatively with closed reduction
- Elbow closed reduction maneuver 1:
- Patient is placed supine and procedural sedation is usually required
- Ask an assistant to provide counter traction at the proximal humerus
- Patient wrist is held with one hand while the dislocated elbow is manipulated from the underside by the other hand
- Reduce any medial/ lateral displacement first by the hand under the elbow
- Then apply traction using both hands with flexion of patient elbow to 90 degrees
- Elbow closed reduction maneuver 2:
- Ask assistant to hold patient wrist and apply traction with flexion
- You hold and push the olecranon distally, anteriorly and medially using your thumbs
- Reduction is confirmed by assessing the full range of motion and varus and valgus stress application while doing that
- After that, the elbow is immobilized in above elbow backslab with 90 degrees of flexion for 1 week and then exercises started
- Repeat radiographs to make sure reduction is good and joint is congruent (joint space equal along the articular surfaces) and repeat neuro examination
- Indications of operative treatment
- Failure of closed reduction
- Joint instability
- Complex fracture dislocations => requires reduction and management of the fractures and damaged soft tissues
- Operative management of elbow injuries usually carries poor prognosis due to secondary osteoarthritis
Complications
- Nerve injury
- Ulnar nerve: most common to be injured with posterior dislocations (neuropraxia)
- Median nerve: maybe entrapped during closed reduction of posterior dislocations
- Radial nerve
- Brachial artery: with anterior dislocations => requires emergency surgery to repair the artery
- Stiffness: loss of 20-30 degrees of terminal extension of the elbow due to prolonged immobilization
- Heterotopic ossification: lead to more stiffness
- Recurrent dislocation: most commonly caused by radial collateral ligament incompetence and fracture dislocation
- Secondary osteoarthritis
Course Menu
This article is apart from The Elbow and Forearm Trauma Free Course; This course contains a number of lectures listed below: